It really represents a very complex mechanism -- the cough reflex arc.
There are cough receptors from the upper airway leading all the way down
to the terminal bronchioles, not including, however, the terminal
bronchioles and the alveoli. There are cough receptors in the nose and
there are cough receptors in the ear canal. So some of you may have had
patients who began coughing when you began doing otoscopic examinations
-- and that's why, because you began stimulating their cough receptors.
These afferent impulses travel via the vagus nerve to the medullary
cough center, and from there a very complex but integrated mechanism
occurs traveling back through efferent vagus nerves that go to the
larynx, the chest muscles, the diaphragm, abdominal wall, pelvic floor,
and the bronchii themselves. And a very complex and very integrated
motor response that leads ultimately to what we see, finally, as the
cough.
http://www.medscape.org/viewarticle/430253
Sunday, January 8, 2012
Dexamethasone suppression test
How the test is performed:
There are two different types of dexamethasone suppression tests: the low-dose test and the high-dose test. Each type can either be done in an overnight or standard (3-day) way.
For the low-dose overnight method, 1 mg of dexamethasone is given at 11 p.m., and the blood is drawn at 8 a.m. for a cortisol measurement (see venipuncture).
In the standard low-dose method, urine is collected 3 days (stored in 24-hour collection containers) for measurement of cortisol. On day 2, a low dose (0.5 mg) of dexamethasone is given by mouth every 6 hours for 48 hours.
For the high-dose overnight method, a baseline cortisol is measured on the morning of the test, then 8 mg of dexamethasone is given at 11 p.m. Blood is drawn at 8 a.m. for a cortisol measurement. For the standard high-dose test, urine is collected over 3 days (stored in 24-hour collection containers) for measurement of cortisol. On day 2, a high dose (2 mg) of dexamethasone is given by mouth every 6 hours for 48 hours.
What abnormal results mean:
If there is not a normal response on the low-dose test, abnormal secretion of cortisol is likely (Cushing's Syndrome). This could be a result of a cortisol-producing adrenal tumor, a pituitary tumor that produces ACTH, or a tumor in the body that inappropriately produces ACTH. The high-dose test can help distinguish a pituitary cause (Cushing's Disease) from the others.
Cushing's syndrome caused by adrenal tumor
There are two different types of dexamethasone suppression tests: the low-dose test and the high-dose test. Each type can either be done in an overnight or standard (3-day) way.
For the low-dose overnight method, 1 mg of dexamethasone is given at 11 p.m., and the blood is drawn at 8 a.m. for a cortisol measurement (see venipuncture).
In the standard low-dose method, urine is collected 3 days (stored in 24-hour collection containers) for measurement of cortisol. On day 2, a low dose (0.5 mg) of dexamethasone is given by mouth every 6 hours for 48 hours.
For the high-dose overnight method, a baseline cortisol is measured on the morning of the test, then 8 mg of dexamethasone is given at 11 p.m. Blood is drawn at 8 a.m. for a cortisol measurement. For the standard high-dose test, urine is collected over 3 days (stored in 24-hour collection containers) for measurement of cortisol. On day 2, a high dose (2 mg) of dexamethasone is given by mouth every 6 hours for 48 hours.
What abnormal results mean:
If there is not a normal response on the low-dose test, abnormal secretion of cortisol is likely (Cushing's Syndrome). This could be a result of a cortisol-producing adrenal tumor, a pituitary tumor that produces ACTH, or a tumor in the body that inappropriately produces ACTH. The high-dose test can help distinguish a pituitary cause (Cushing's Disease) from the others.
Cushing's syndrome caused by adrenal tumor
- Low dose: no change
- High dose: no change
- Low dose: no change
- High dose: no change
- Low dose: no change
- High dose: normal suppression
Saturday, January 7, 2012
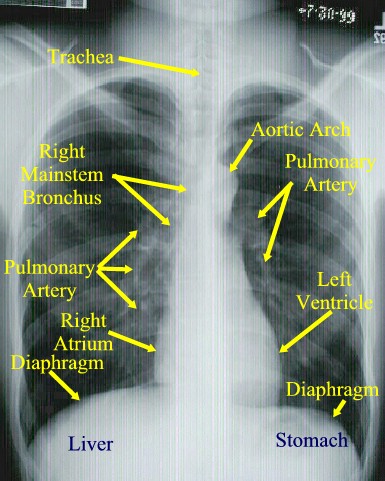
What is the main constituent of the hilar shadows seen radiographically?
The hilar shadows seen on radiography are caused mainly by branches of the pulmonary arteries, although the larger bronchi can frequently be recognized.

http://www.dartmouth.edu/~humananatomy/part_4/chapter_22.html
http://www.dartmouth.edu/~humananatomy/part_4/chapter_22.html
Subscribe to:
Comments (Atom)